

Powerful mechanical thrombectomy performance
Simple set-up
Saline jets travel backwards at high speed to create a negative pressure zone (less than -600 mmHg) causing a powerful vacuum effect
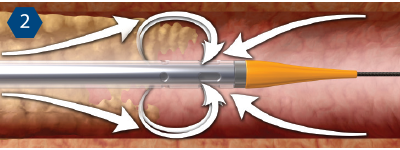
Cross-StreamTM windows optimize the fluid flow for more effective thrombus removal.

Thrombus is drawn into the catheter where it is fragmented by the jets and evacuated from the body.
Only Boston Scientific supplies thrombectomy solutions for every level of thrombus burden, with proven performance and minimal complications.
SPIROFLEX™ ANGIOJET thrombectomy of a native coronary artery in a patient presenting with a ST elevation myocardial infarction (STEMI) due to stent thrombosis.
Patient History
Patient was referred for coronary angiography
Diagnostic Angiogram
Occluded RCA Acute Stent Thrombosis
Procedure
Post ANGIOJET
Definitive Treatment
Following PTCA with stenting, final TIMI flow was 3; final thrombus grade was 0.
Physician Commentary
As in this case, patients presenting with recurrent thrombosis over a long stented segment often have a large thrombus burden.
The ANGIOJET Thrombectomy System is ideal to treat patients with a considerable amount of large thrombus and in this patient the ANGIOJET successfully removed a significant thrombus from the mid and distal RCA making definitive treatment easier and reestablishing TIMI 3 flow.
This case demonstrates the utility of mechanical thrombectomy with the ANGIOJET SYSTEM in a patient presenting with a STEMI secondary to stent thrombosis and a substantial thrombus burden in the culprit vessel.
Final Result Post Definitive Treatment
Study and cines courtesy of Jeffrey Chambers, MD, Metropolitan Heart and Vascular Institute, Minneapolis, MN. Results from case studies are not predictive of results in other cases. Results in other cases may vary.
Fifth Floor, Krishna Apra Business Square, Netaji Subhash Place, Pitampura, Delhi-110034
+91 -11 - 45110111
info@acecardiopathy.com
Get updates for our all products.
© 2021 Ace Cardiopathy. All rights reserved. Design and Developed by Easy Solution 360.